Ghada Bassioni, Ain Shams University
If you’re baking fish, roasting vegetables or preparing a piece of meat for dinner tonight, chances are that you’ll wrap your food in aluminium foil. What you may not realise is that some of the foil will leach into your meal – and this could be bad for your health.
Research that I conducted with a group of colleagues has explored the use of aluminium for cooking and preparing food. Aluminium doesn’t just appear in foil: it is the most popular cookware material used by people in developing countries. Pots and pans are lined with it and it is found in some kitchen utensils like large serving spoons. Copper used to fulfil this role, but over time it’s been replaced by aluminium because it is cheaper to mass produce and easier to clean.
But while cooking your food in aluminium pots or pans isn’t a bad thing, placing it in foil and putting it in the oven is problematic. This is especially true with acidic or spicy food that’s prepared at high temperatures.
Aluminium and health
Human bodies can excrete small amounts of aluminium very efficiently. This means that minimal exposure to aluminium is not a problem: the World Health Organisation has established a safe daily intake of 40mg per kilogram of body weight per day. So for a person who weighs 60kg the allowable intake would be 2400 mg.
But most people are exposed to and ingest far more than this suggested safe daily intake. Aluminium is present in corn, yellow cheese, salt, herbs, spices and tea. It’s used in cooking utensils, as described above, as well as in pharmacological agents like antacids and antiperspirants. Aluminium sulfate, which is derived from aluminium, is used as a coagulant during the purification process of drinking water.
Scientists are exploring whether over-exposure to aluminium may be posing threats to human health. For instance, high concentrations of aluminium have been detected in the brain tissue of patients with Alzheimer’s disease. Scientists have examined the community of old people with Alzheimer’s and concluded that it is a modern disease that’s developed from altered living conditions associated with society’s industrialisation. These conditions may include high levels of aluminium in daily life.
Aluminium poses other health risks, too. Studies have suggested that high aluminium intake may be harmful to some patients with bone diseases or renal impairment. It also reduces the growth rate of human brain cells.
Avoid foil when cooking
Given all of these proven risks, it’s important to determine the aluminium concentration when cooking. Pots and other cookware tend to be oxidised, providing an inert layer that prevents the aluminium from leaching into food. The problem is that when you scrub your pots after cooking, that layer is worn away and the aluminium can seep into your food. This is easily avoided: when you get new aluminium pots, boil water in them several times until the base becomes matt. This creates a natural oxidation that prevents leaching. They may look nicer when they’re scrubbed and shiny, but a matt base is better for your food and your health.
But cooking your food in foil is a different story. Aluminium foil is disposable and you will not be able to create that inert layer prior to using it. My research found that the migration of aluminium into food during the cooking process of food wrapped in aluminium foil is above the permissible limit set by the World Health Organisation.
Ghada Bassioni explains the research she and her colleagues conducted.
Aluminium is significantly more likely to leach into food, and at higher levels, in acidic and liquid food solutions like lemon and tomato juice than in those containing alcohol or salt. Leaching levels climb even more when spice is added to food that’s cooked in aluminium foil. Anything acidic sparks a particularly aggressive process that dissolves layers of aluminium into food.
This research suggests that aluminium foil should not be used for cooking. Instead, we’d recommend using glassware or porcelain when preparing baked dishes. It’s safe to wrap cold food in foil, though not for long stretches of time because food has a shelf life and because aluminium in the foil will begin to leach into the food depending on ingredients like spices. Ghada Bassioni, Associated Professor and Head of the Chemistry Department, Ain Shams University
This article was originally published on The Conversation. Read the original article.
Stephen Euston, Heriot-Watt University
So much for the decades in which fats and oils were public enemy number one on our dinner plates. There is more and more evidence that sugar – or more precisely, carbohydrate – is behind our increasing rates of obesity and heart disease. Even if the mechanisms by which this occurs are still not well defined, there are endless calls for reducing its quantities in the foods we eat. Most recently in the UK this led to the chancellor, George Osborne, announcing a tax on sugary soft drinks.
Had we ever come up with a proper substitute for sugar, of course, we wouldn’t need to have this debate. In our sweetness-addicted era, it is one of science’s greatest challenges. So why has it eluded us for so long, and are we any closer to a solution?
Saccharine on saleLunasee Studios
Replacing the sweetness of sugar in foods is actually relatively straightforward. The first synthetic sweetener, saccharine, was discovered accidentally by a young Russian chemist named Constantin Fahlberg in 1879 while studying coal-tar derivatives, when he unknowingly got it on his hands and licked his fingers. Saccharine became widely used around World War I, when natural sugar was in short supply. In the 1960s scientists discovered several more artificial sweeteners in similarly serendipitous ways, including aspartame and acesulfame K.
As well as these discoveries, there are naturally occurring sweeteners that we have actually known about for much longer (see table below). The Guarani peoples of modern-day Brazil and Paraguay have been using the leaves of the stevia plant as a sweetener for about 1,500 years. And the seeds of the West African katemfe fruit, which contain a sweet chemical called thaumatin, have been on our radar since the 19th century.
‘Sweetness’ is relative to sugar – stevia is 275 times as sweet.
Sweet but sour
Yet while we have plenty of options for sweetness, there are several difficulties associated with using non-sugar sweeteners in foods. There have been various cancer scares over the years, which have affected stevia, saccharine and aspartame, among others. Some artificial sweeteners have also been linked to type 2 diabetes.
To compound this, governments class all non-sugar sweeteners as additives, which means they are assigned an E-number – even stevia and thaumatin. In an era where consumers have become increasingly wary of these numbers even when there aren’t specific health risks, manufacturers have been moving towards so-called “clean-label” products that are free of them. This puts these sweeteners at a disadvantage.
Aside from health and labelling, sugars have chemical functions in foods that make them difficult to replace. Sugar solutions freeze at a lower temperature than pure water, for instance. In products like ice cream, this is critical to maintaining a soft texture at freezer temperatures.
Sugars play an important role in giving products like bread, cakes and even wine their darker colour, through what chemists call non-enzymatic browning reactions. Artificial
sweeteners are not good at reproducing either of these.
‘Mmmm aspartame.’Monkey Business Images
Then there is aftertaste. This arises from the mechanism by which sweetness is detected in the taste buds. One problem is that the structural features of any sweet molecule that allow them to bind to the sweetness receptors on the tongue are similar to the ones that bind to our bitterness receptors. This is why some sweeteners leave a bitter aftertaste, which is of course undesirable to some consumers.
But looking at the previous table again, for sweeteners that don’t have a bitter aftertaste there is another issue. Artificial sweeteners bind more strongly to the sweetness receptors and have a different and longer-lasting taste profile to sugar, and so are perceived as tasting different by consumers.
All in all, although non-sugar sweeteners are a multi-billion-pound industry, these drawbacks help to explain why they are nowhere near eclipsing sugar. In 2014 sugar (sucrose) accounted for 78% of all sweetener sales. Artificial sweeteners made up 8%, with acesulfame k the market leader. Natural alternatives like stevia, which was banned in the US and EU until fairly recently, made up 1%. (The rest of the market comprises everything from glucose to syrups).
Where sweeteners go from here
The cancer evidence against non-sugar sweeteners has turned out to be thinner than feared. Cancer Research UK and the US National Cancer Institute both say there is no increased risk regarding artificial sweeteners. Stevia’s years in the wilderness were the result of an anonymous complaint about the cancer risks to the US authorities commonly thought to have come from artificial-sweetener producers, but it has since been rehabilitated. As for type 2 diabetes, the evidence linking it to artificial sweeteners is inconclusive and we need more research – so far it has all been done on animals.
On the physical issues, food scientists have had to think creatively. When it comes to texture, for instance, manufacturers add protein texturisers instead – soy, for example. Or you can turn to other substances that have a similar effect as sugar on the freezing properties of water – the sugar alcohol erythritol is one option.
Stevia wonder?Olivier le Moal
Manufacturers seek to overcome the aftertaste issue by mixing sweeteners. We perceive the aftertaste of different sweeteners over differing timescales, so one sweetener can be used to mask the aftertaste of a second. It is common to use stevia in combination with acesulfame K, for instance.
Another increasingly common ploy is to mix sugar and other sweeteners together. This helps explain why the use of non-sugar sweeteners in new product launches rose from 3.5% in 2009 to 5.5% in 2012. It also explains why stevia is rocketing. Food analysts Mintel and Leatherhead forecast it will have become the most widely used non-sugar sweetener by as early as next year.
In the absence of a Holy Grail for sugar replacement, this could be as good as it gets any time soon. No wonder the authorities are beginning to intervene to save us from our sweet tooth instead. Stephen Euston, Professor, Heriot-Watt University
This article was originally published on The Conversation. Read the original article.
‘Benidorm, Spain’ drawn in 1979 by Richard Wawro. MIke Wawro
Joanne Ruthsatz, The Ohio State University
As a toddler growing up in the 1950s, Richard Wawro threw violent tantrums. Often, he would tap the same piano key for long stretches of time.
When he was three, his parents took him for testing at a nearby hospital. They were told that he was moderately to severely retarded. His family, however, never believed that his IQ was as low as the experts claimed.
A special education teacher began working with Richard when he was six. She introduced him to drawing with crayons, which he took to quickly.
He began filling sketchbooks (and the wallpaper of his Scotland home) with startlingly accurate depictions of cartoon characters like Yogi Bear. When Richard was 12, his artwork astounded a visiting artist who said that his drawings were created “with the precision of a mechanic and the vision of a poet.”
Richard could never read or write well. His speech remained limited. But his involvement with the art world spurred his social development. He participated in dozens of exhibitions and became a well-known artist. His artwork was celebrated by the media and in a documentary, “With Eyes Wide Open.” Both Margaret Thatcher and Pope John Paul II owned Wawro’s originals.
Richard was a savant, an individual with a spike in a particular ability combined with an impairment or disability. In Richard’s case, that underlying condition was autism. Autism is a condition characterized by social and communication challenges, like difficulty making eye contact or making conversation, along with repetitive behaviors or intense interests.
It turns out that many savants have autism. In a 2015 paper, the savant expert Darold Treffert reported that among the congenital savants in his registry, 75 percent had an autism spectrum disorder, a term used to describe a group of disorders with variable symptoms and severity.
Exceptional memory and autism
Not every autistic individual has extraordinary talents.
In fact, autism can be accompanied by serious challenges that last a lifetime (as was also the case for Wawro, whose family handled his daily living needs until he died at age 53).
But when the astounding abilities are there, they are often rooted in extreme memory, excellent attention to detail and passionate interests – traits also linked to autism.
Many autistic kids show exceptional abilities.Valary, CC BY-NC-ND
My work has been with child prodigies, those astounding individuals who perform at an adult-professional level in a demanding field before adolescence.
In many ways, prodigies look a lot like savants. They have the same preternatural abilities. They have the same prolific output.
But there’s a key difference between the two. While in savants, these extreme abilities are paired with an underlying impairment or disability, prodigies don’t typically have any such disability.
Still, as I recount in my new book, The Prodigy’s Cousin, I have found the overlap between prodigy and autism to be striking. Even though prodigies are not typically autistic, they have the same excellent memories, extreme attention to detail, and passionate interests linked to autism and autistic savants.
The prodigies' excellent memories were almost immediately apparent. When I investigated nine prodigies across twostudies, each one scored in the 99th percentile for this ability. When this group was expanded to 18 prodigies in a 2014 study, the prodigies’ average working memory score was 140 – north of the 95th percentile.
Early work on autism
Reports linking extreme memory and autism date back to the first published reports of Leo Kanner and Hans Asperger, the two scientists credited with identifying autism as an independent condition in the 1940s.
In his landmark 1943 study, Kanner remarked upon his subjects’ “excellent memory for events of several years before, the phenomenal rote memory for poems and names, and the precise recollection of complex patterns and sequences.”
Memory in autistic kids is complex.mimitalks, married, under grace, CC BY-NC-ND
He included a report of a boy, Donald T., with “an unusual memory for faces and names,” who had memorized “an inordinate number of pictures in a set of Compton’s Encyclopedia.” Another, Charles N., could distinguish between 18 symphonies at age one-and-a-half.
Since Kanner’s time, scientists have found that memory in autism is complex. But in a 2015 study, a team of researchers found that more than half of their 200 autistic subjects had notable memories. Treffert has described excellent memory as “integral” for savants in particular.
Prodigies and autism
As part of my 2012 study, the child prodigies I worked with were given the Autism-Spectrum Quotient, a self-administered test designed to measure autistic traits. On attention to detail, they outscored not only the controls, but also those with an autism spectrum disorder.
Attention to detail is another strength associated with autism. Some have described excellent attention to detail as “a universal feature of the autistic brain.” In 2006, the prominent autism researchers Francesca Happé and Uta Frith concluded that there was strong evidence that autism was associated with superiority on “tasks requiring detail-focused processing.”
Child prodigies are also exceptionally passionate about their area of expertise.
Such passionate interests are closely associated with autism. They are even part of autism’s diagnostic criteria.
This trait has been observed since the early days of autism research. Kanner’s 1943 paper includes a description of Alfred L., a child whose mother noted his tendency toward intense interests. As she put it:
He talks of little else while the interest exists, he frets when he is not able to indulge in it (by seeing it, coming in contact with it, drawing pictures of it), and it is difficult to get his attention because of his preoccupation.
This sort of passion can result in prolific output, as it did for Richard Wawro, who created at least 2,453 pictures in his lifetime.
Why do prodigies have autistic relatives?
The link between prodigy and autism could be even deeper than we think.
Researchers have found that child prodigies often have an autistic relative.hepingting, CC BY-SA
In addition to drawing from a similar well of cognitive abilities, there appears to be a family link between prodigy and autism. In a study I conducted in 2012, more than half of the prodigies investigated had a close autistic relative. In one instance, a prodigy had five autistic relatives.
Another study I conducted with colleagues at The Ohio State University suggests that prodigies and their autistic relatives may even share a genetic link. We found evidence that the prodigies and their autistic relatives both had a mutation on chromosome one not shared by their non-prodigious, non-autistic relatives.
The same traits that are celebrated in prodigies – like their excellent attention to detail and the passionate interests – are often recognized as strengths in the context of autism, too, though sometimes families report that the extreme nature of autistic interests can take a toll on family life.
This is a real challenge, as are other aspects of autism. Figuring out the best way to support those with autism and their families is essential.
But let’s remember the strengths of autism as well as the challenges. Kimberly Stephens, coauthor of The Prodigy’s Cousin, contributed to this piece. Joanne Ruthsatz, Assistant Professor of Psychology, The Ohio State University
This article was originally published on The Conversation. Read the original article.
Lab results confirm a new case of Ebola virus disease in Liberia — a 30-year-old woman who died yesterday afternoon while being transferred to a hospital in the capital Monrovia.
Liberia’s Ministry of Health, WHO and partner agencies immediately sent a team to the community outside Monrovia where the woman lived and the clinic where she was being treated to begin case investigation and identification of individuals who may have been in contact with her.
Liberian health authorities convened an emergency meeting early this morning with key partners to coordinate and plan a rapid response.
This latest case marks Liberia’s third flare-up of Ebola virus disease since its original outbreak was declared over on 9 May 2015. The last flare-up in the country began in November 2015 and ended 14 January 2016. Neighbouring Guinea is also responding to a new cluster of Ebola cases in its southern prefecture of Nzérékoré.
Earlier this week, at the recommendation of the International Health Regulations Emergency Committee, WHO declared that the Ebola epidemic in West Africa no longer represents a Public Health Emergency of International Concern. WHO said Guinea, Liberia and Sierra now have the detection and response capacities in place to effectively manage ongoing flare-ups of Ebola, pointing to the swift response and rapid containment of recent small outbreaks.
But WHO reiterated that additional flare-ups of the disease are expected in the months to come, largely due to virus persistence in some survivors, and that the three countries must remain on high alert and ready to respond. WHO has maintained close to 1,000 experienced staff in the region who are ready to contribute to emergency response operations if needed, while working to recover and strengthen health systems in the three countries.
An Ebola training exercise at Madigan Army Medical Center’s Andersen Simulation Center, in the US. John Liston/Army Medicine/ flickr
David Sanders, University of the Western Cape This article is a foundation essay. These are longer than usual and take a wider look at a key issue affecting society.
The global health threats posed by recent viral epidemics, such as avian flu, H1N1, Ebola and Zika, have been happening too frequently to be dismissed as coincidental.
Unless the global public health community invests in and develops better health systems that provide for the poor, such viruses will continue to spread and have severe effects.
The mosquito-borne Zika virus was declared a global public health emergency by the World Health Organisation in February 2016 due to an increase in the number of microcephaly cases in areas where the virus was found. Microcephaly is a birth defect where babies are born with abnormally small heads. A causal link between in-utero exposure to the Zika virus and microcephaly has not yet been proven.
This is the first time since the Ebola epidemic hit Africa in 2014 that the World Health Organisation has declared a global health emergency. Although the speed with which the organisation reacted has been welcomed, mounting an emergency response is not sufficient to manage the spread of viral epidemics like that of Zika.
In the case of the Ebola outbreak, after a long delay, the World Health Organisation called for an urgent change in three main areas. These included:
rebuilding and strengthening national and international emergency preparedness and response;
addressing the way new medical products are brought to market; and
strengthening the way in which the World Health Organisation operates during emergencies.
But the response has not been far-reaching enough to prevent similar viral outbreaks. The Zika virus is proof of this. Environmental, social and economic factors cause populations not previously affected by a particular disease to be exposed to its virus. To tackle such outbreaks in future, these factors must be addressed.
Containing the spread of a virus
Outbreaks happen for two reasons: the daily conditions that negatively affect the health of a country’s inhabitants have not been addressed; and there are weak national health systems in place. There are several structural drivers that influence these, resulting in outbreaks and determining their severity. These include:
the way populations move and migrate. This is compounded by generally poor access to (weak) health-care services, especially for migrant populations.
hybrid viruses that appear in food processing factories and increase the chances of human-animal interactions.
increased interaction between human and forest animals. This happens as indigent populations are forced deeper into forested areas to look for food.
A transmission electron micrograph of the Ebola virus.Frederick A Murphy/ CDC Global/ flickr
This increased interaction is thought to be behind the spread of Ebola. Human beings were never the primary target of the virus. It is believed the virus was primarily found in a few species of fruit bats, which live in the tropical rainforests of central Africa.
Although central Africa has been the site of all earlier major Ebola outbreaks, it is hundreds of kilometres from the epicentre of the latest epidemic, which took place in West Africa. The geographic spread may be explained by poverty forcing people deeper into the forests in search of food, where they came into contact with the fruit bats or other animals infected by the bats.
How is the recent explosive Ebola outbreak explained? The answer lies not in the pathology of the disease but in the pathology of society, and the global political and economic architecture.
Economic exploitation is partly to blame
The spread of the Ebola epidemic was the result of poverty and the ruthless exploitation of the region’s natural resources. Those afflicted, at least initially, were typically the poorest – those forced, by scarcity, to look for food in the forests, where they came into contact with animals harbouring the virus.
Economic exploitation also resulted in under-resourced and weak health systems that could not contain the spread of the virus.
Take Sierra Leone, for instance. Its iron ore mining industry has rapidly expanded, fuelling economic growth in the country of 20% in 2013, according to the International Monetary Fund. Interest in its largely untapped mineral resources sparked a flood of investment a decade after the end of the devastating 1991 to 2002 civil war. The country’s economic growth rate is ranked among the highest in the world.
Yet in 2010 the country’s mining industry contributed almost 60% of exports but only 8% of government revenue. In 2011, only one of the major mining firms in the country was paying corporate income tax, while none of the top five was reporting profits despite a boom in mineral exports.
Similarly, both Liberia and Guinea have been heavily targeted by foreign companies. Liberia currently has the highest ratio of foreign direct investment to gross domestic product in the world. This largely is the result of foreign ownership of rubber production companies.
In Guinea, the area affected by Ebola attracted agribusiness shortly before the outbreak. In 2010, the British-backed Farm Land of Guinea Limited bought huge tracts of land for maize and soybean cultivation. And an Italian energy company has bought more than 700,000 hectares for biofuel crops.
These countries’ dependence on extractive industries such as mining and logging, and financial losses due to tax evasion have left them impoverished and contributed to under-investment in – and the severe weakness of – their health systems.
Weak health systems
Volunteer burial teams in Guinea disinfect themselves after carrying the body of an Ebola victim.UN Photo/Martine Perret
It is no accident that the Ebola epidemic affected three of the poorest countries in the world.
Liberia, Guinea and Sierra Leone number 175, 179 and 183, respectively, out of 187 countries on the United Nations’ Human Development Index. Their health systems are ineffective and almost nonexistent in many regions, affecting management of diseases.
In Sierra Leone, for example, in the four months following the outbreak of Ebola, 848 people were infected by the virus and 365 died. And in an average four months, the country sees about 650 deaths from meningitis, 670 from tuberculosis, 790 from HIV/AIDS, 845 from diarrhoea and more than 3,000 from malaria.
Such deaths have been occurring for decades, but with no previous focus on these countries.
Furthermore, in these three countries there is a persistent crisis of human resources, with a serious deficit of health workers, especially in rural areas. This is a result of long-term underproduction and continuing migration. More Liberian and Sierra Leonean medical doctors work in the US and UK than in their home countries.
How to solve the problem
As a start, it is important to focus on crisis response. The World Health Organisation had a feeble initial response to Ebola, in part, because of cuts of more than 50% in its outbreak and response budget – the very budget line needed to respond to Ebola. This dropped from US$469 million in 2012/2013 to US$228 million in 2014/2015, mainly because member states, particularly rich ones, failed to pay their financial contributions.
But managing viral epidemics requires that authorities look beyond the immediate crisis response. A major and sustained investment in human resources is required. Initially, this will require greatly increased donor assistance.
In the medium term, there is an urgent need to strengthen health systems in the region. Although talk of “health systems strengthening” has become commonplace there is little evidence of this in several African countries.
But the most sustainable solution requires fundamental changes to economic and power relations between these countries and the capitalist economies and enterprises that continue to bleed them dry, often with the collusion of local officials and elites. Amit Sengupta, associate co-ordinator of the People’s Health Movement, was involved in the formulation of this article.
Marco Springmann, University of Oxford
Eating more fruit and vegetables and cutting back on red and processed meat will make you healthier. That’s obvious enough. But as chickens and cows themselves eat food and burn off their own energy, meat is a also major driver of climate change. Going veggie can drastically reduce your carbon footprint.
This is all at a personal level. What about when you multiply such changes by 7 billion people, and factor in a growing population?
In our latest research, colleagues and I estimate that changes towards more plant-based diets in line with the WHO’s global dietary guidelines could avert 5m-8m deaths per year by 2050. This represents a 6-10% reduction in global mortality.
Food-related greenhouse gas emissions would also be cut by more than two thirds. In all, these dietary changes would have a value to society of more than US$1 trillion – even as much as US$30 trillion. That’s up to a tenth of the likely global GDP in 2050. Our results are published in the journal PNAS.
Future projections of diets paint a grim picture. Fruit and vegetable consumption is expected to increase, but so is red meat consumption and the amount of calories eaten in general. Of the 105 world regions included in our study, fewer than a third are on course to meet dietary recommendations.
A bigger population, eating a worse diet, means that by 2050 food-related GHG emissions will take up half of the “emissions budget” the world has for limiting global warming to less than 2℃.
To see how dietary changes could avert such a doom and gloom scenario, we constructed four alternative diets and analysed their health and environmental impacts: one reference scenario based on projections of diets in 2050; a scenario based on global dietary guidelines which includes minimum amounts of fruits and vegetables, and limits to the amount of red meat, sugar, and total calories; and two vegetarian scenarios, one including eggs and dairy (lacto-ovo vegetarian), and the other completely plant-based (vegan).
Millions of avoidable deaths
We found that adoption of global dietary guidelines could result in 5.1m avoided deaths per year in 2050. Vegetarian and vegan diets could result in 7.3m and 8.1m avoided deaths respectively. About half of this is thanks to eating less red meat. The other half comes thanks to eating more fruit and veg, along with a reduction in total energy intake (and the associated decreases in obesity).
There are huge regional variations. About two thirds of the health benefits of dietary change are projected to occur in developing countries, in particular in East Asia and South Asia. But high-income countries closely follow, and the per-person benefits in developed countries could actually be twice as large as those in developing countries, as their relatively more imbalanced diets leave greater room for improvement.
Room for improvement.Lightspring / shutterstock
China would see the largest health benefits, with around 1.4m to 1.7m averted deaths per year. Cutting red meat and reducing general overconsumption would be the most important factor there and in other big beneficiaries such as the EU and the US. In India, however, up to a million deaths per year would be avoided largely thanks to eating more fruit and vegetables.
Russia and other Eastern European countries would see huge benefits per-person, in particular due to less red meat consumption. People in small island nations such as Mauritius and Trinidad and Tobago would benefit due to reduced obesity.
Vegans vs climate change?
We estimated that adopting global dietary guidelines would cut food-related emissions by 29%. But even this still wouldn’t be enough to reduce food-related greenhouse gas emissions in line with the overall cutbacks necessary to keep global temperature increases below 2°C.
India could cut its emissions and save lives – at the same time.Christopher Fynn, CC BY
To seriously fight climate change, more plant-based diets will be needed. Our analysis shows if the world went vegetarian that cut in food-related emissions would rise to 63%. And if everyone turned vegan? A huge 70%.
What’s it worth?
Dietary changes would have huge economic benefits, leading to savings of US$700-1,000 billion per year globally in healthcare, unpaid informal care and lost working days. The value that society places on the reduced risk of dying could even be as high as 9-13% of global GDP, or US$20-$30 trillion. Avoided climate change damages from reduced food-related greenhouse gas emissions could be as much as US$570 billion.
Putting a dollar value on good health and the environment is a sensitive issue. However, our results indicate that dietary changes could have large benefits to society, and the value of those benefits makes a strong case for healthier and more environmentally sustainable diets.
The scale of the task is clearly enormous. Fruit and vegetable production and consumption would need to more than double in Sub-Saharan Africa and South Asia just to meet global dietary recommendations, whereas red meat consumption would need to be halved globally, and cut by two thirds in richer countries. We’d also need to tackle the key problem of overconsumption. It’s a lot to chew on. Marco Springmann, Researcher, University of Oxford
This article was originally published on The Conversation. Read the original article.
Bob Patton, University of Surrey
The UK’s new alcohol guidelines advise that men and women shouldn’t drink more than 14 units of alcohol a week. Previous advice for the British drinker presented a higher threshold for men, so this represents a considerable change. So what was the evidence that the limits should not take gender into account?
Most countries that provide guidelines on alcohol consumption suggest higher threshold levels for men than women. It is well known that, physiologically, women are more vulnerable to the toxic effects of alcohol than men. Pint for pint, women have a greater risk of alcohol related problems such as dependency, certain cancers (liver, mouth and stomach) and other physical and psychological health issues.
A complex interplay of genetics, environment, personality and motivation contributes towards the likelihood of experiencing these conditions. The different risk factors faced by men and women are particularly apparent at higher levels of consumption – what we now call “drinking with increasing risk”. That is, men who regularly drink more than three or four units a day and women who regularly drink more than two or three units a day. But at levels of consumption lower than this, these differences are not as clear cut.
Drinking with increasing risk.www.shutterstock.com
An acceptable risk
The latest guidelines are based on data provided by the University of Sheffield. It shows that anyone who drinks every day and who consumes no more than 14 units of alcohol a week has a less than one percent chance of dying from an alcohol-related health condition at any time.
One percent was adopted by the guidelines committee as the maximum level of risk that would be acceptable to the public. This has been presented as a similar level of risk to the chance of dying in a car accident. (In fact, the chances of dying in a road accident are even smaller – at less than 0.5% over a lifetime.) But most people don’t drink every day and so, for the majority, the situation is a little less clear cut.
So it’s not just how much, but also how often, we drink that counts, with decreasing frequency associated with increased risk. The Sheffield data shows that men drinking 14 units a week on a single occasion have a 4.5% lifetime risk of dying from an alcohol-related health condition. For women drinking at the same level on a single occasion each week, the risk is 2%.
Interestingly, at the new guideline threshold, men have an almost five times (0.99%) greater risk of death than women (0.18%), but still less than 1% overall. If we consider the previous threshold of 21 units a week for men drinking seven days a week, the risk of alcohol-related death increases to 3%. Complicated, isn’t it?
The new guidelines present the message that there is no “safe” level of alcohol consumption but stop short of recommending abstention as the best policy. In fact, the Sheffield data shows that for both men and women drinking up to seven units a week, spread across three or more days, actually has a protective effect on death from an alcohol-related health condition. For men the benefit is very small (a 0.1% improvement), compared with over 2% for women.
A better way to present the data
Given that there are well established and significant differences between male and female responses to alcohol across a range of quantities and frequencies of consumption, it is difficult if not impossible to encompass this diversity into a single recommendation of what represents the optimal limits of consumption with regard to the likelihood of dying from an alcohol related condition.
It might be better to present information on the relative risks associated with increasing use. This allows a comparison with non-drinkers, for example: “Men who regularly drink five units a day have a threefold increased risk of death from cirrhosis of the liver compared with non-drinkers.” In fact, the expert committee that helped to put the guidelines together noted that this might have been a better way to illustrate the relationship between drinking and death.
The situation is complex. Although it’s clear that there are benefits to both health and society by reducing alcohol consumption, the reasoning behind the cut-off of 1%, as an acceptable level of risk, or the underlying assumption that those who drink do so on a daily basis, is unclear.
While the guidelines set out to provide helpful advice about drinking, ignoring the differences between male and female responses to alcohol, is a risky strategy. If the guidelines don’t resonate with those of us who choose to drink, they will simply be ignored, and that won’t do anyone any good at all.
Two tobacco giants are seeing strong demand for their reboots of the e-cigarette in Japan, with Philip Morris International (PM.N) twice postponing a nationwide rollout and Japan Tobacco (2914.T) suspending shipments - both due to supply shortages.
Japan has become a key testing ground for the two companies and their new, real tobacco e-smokes as they grapple with shrinking demand for traditional cigarettes in other developed countries.
Philip Morris, the world's largest tobacco company, has postponed the nationwide rollout of its iQOS to April 18.
"We believe that the success of iQOS commercialization in Japan will accelerate its global expansion," Philip Morris Japan president Paul Riley told Reuters.
Japan Tobacco CEO Mitsuomi Koizumi told an earnings briefing in February: "We have very high expectations for growth of the so-called tobacco vapor category in five years or so from now."
The iQOS is a tobacco stick that is heated just enough to produce an aerosol but not combust. The company is betting the presence of real tobacco will make it more satisfying to smokers than existing e-cigarettes.
The new device, priced at 9,980 yen ($89), appears similar to other e-cigarettes in that it is pen-shaped and battery-powered, and is heated to release tobacco vapor.
A key distinction is the refills, sold as Marlboro HeatSticks. Most e-cigarettes sold elsewhere use nicotine-laced liquid, which is heavily regulated in Japan. A pack of 20 HeatSticks sells for 460 yen, the same as regular Marlboro cigarettes.
Philip Morris has introduced the products in major cities in Switzerland, Italy and other countries, but Japan is the first country it plans a nationwide release.
The company had originally planned to sell the product throughout Japan on March 1, but postponed the launch to the end of the month due to a potential supply shortage after it saw stronger-than-expected sales in 12 prefectures where it has been test marketing.
The company estimates the market share of Marlboro HeatSticks reached 2.4 percent in Tokyo at the end of January.
Japan Tobacco, which commands about 60 percent of Japan's cigarette market and is the world's third-largest tobacco maker, has also got in on the action by acquiring two overseas e-cigarette makers in the past two years.
In Japan, it has launched the Ploom TECH, priced at 4,000 yen and sold with 460-yen packs of five capsules. Ploom TECH's selling point is that vapor generated from a liquid cartridge passes through the capsules' granulated tobacco, creating a taste the company says is close to the real thing.
"There is definitely a need for products that are smokeless but are still satisfying as cigarettes," said Masanao Takahashi, director at Japan Tobacco's emerging products marketing division.
Like iQOS, Ploom TECH's initial launch in the southern Japanese city of Fukuoka proved so popular that the shipment of the device were suspended after a week due to a supply shortage.
It is currently working on a nationwide launch and is also eyeing a global expansion later this year.
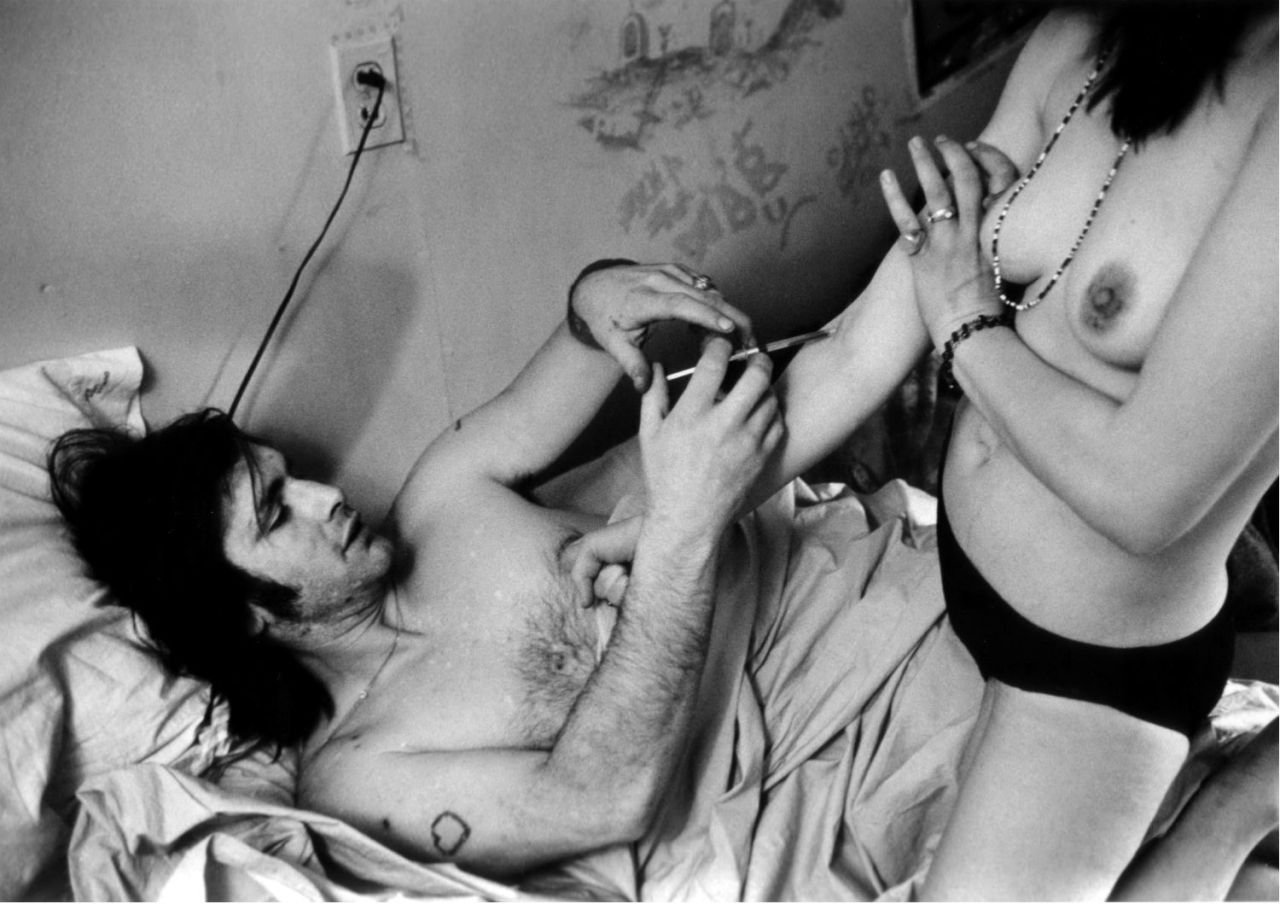
For over a year, I’ve been documenting the lives of three long-term drug users – Marie, Cheryl and Johnny – who are participating in Vancouver’s heroin-assisted clinical study and program.
In recent years, heroin use in North America has exploded into an “epidemic.” At the same time, policymakers and the public have clashed over how to properly treat this public health scourge. Many heroin users receive methadone and other forms of treatment. However, some of the most vulnerable addicts haven’t responded to medication and detox.
I spent weeks building a rapport and trust with Marie, Cheryl and Johnny, who’ve all been addicted to heroin for years. They’ve each repeatedly tried detox and methadone and have been unable to stop using heroin.
In a sense, heroin-assisted treatment, a science-based, compassionate approach, is their last resort.
Those involved in the program – often users who haven’t sufficiently responded to other forms of treatment – receive pharmacological heroin in a clinical setting. While these programs have long been recognized as scientifically sound and cost-saving in countries like Switzerland, the Netherlands and Denmark, heroin-assisted treatment is only beginning to be offered in North America.
At first, the three subjects allowed me to take photos of them self-injecting their medication at Providence Health Care’s Crosstown Clinic in Vancouver’s Downtown Eastside. Slowly, over a period of weeks and months, they let me document their lives outside the clinic.
While I hoped to inform the public about heroin-assisted treatment, I also wanted to see if I could create visual counter-narratives to challenge the dominant tropes of drug genre photography.
More than anything, I wanted to represent Marie, Cheryl and Johnny as human beings – and show that their drug use didn’t define who they were, even though that’s how heroin users are usually depicted by documentary and news photographers.
The best way to do this, I realized, was to show them the photographs I’d selected and give them the opportunity to respond. I included their words with each photograph in the series.
‘Dark, seedy, secret worlds’
Before beginning my project, I had explored the work of some of the most influential drug genre photographers, and found that most of them have consistently represented heroin users as exotic, primitive and dangerous to society.
“There is a tendency in drug photography to attempt to make images of dark, seedy, secret worlds,” writes criminologist John Fitzgerald.
This can have the effect of “othering” the subjects – the idea that after looking at these kinds of images, viewers might look at drug users as outcasts.
Larry Clark’s 1971 photo work “Tulsa” is considered an exemplar of documentary photography. Many view the series, which depicts teenagers experimenting with drugs, sexuality and guns, as brutally honest and revealing.
In this photograph from his seminal work ‘Tulsa,’ photographer Larry Clark eroticizes the risky behavior of teens.Larry Clark, 'Couple,' Tulsa, 1971.
Clark’s follow-up photo essay, “Teenage Lust,” published in 1983, also focused on drug users in a voyeuristic, unsettling and erotic way.
The problem with this approach is that it creates sensationalized images, which, in turn, influence the public’s thinking and policymakers' decisions about how to treat drug users.
“For Clark the drug user is a modern primitive,” writes Fitzgerald. “Like the young boys who play with guns and explore their sexuality, Clark’s drug users plumb the depths of rapacious desire, so repressed and unexplored in the modern body. Clark’s lifework is to bring this primitive desire to light in a liberal artistic adventure.”
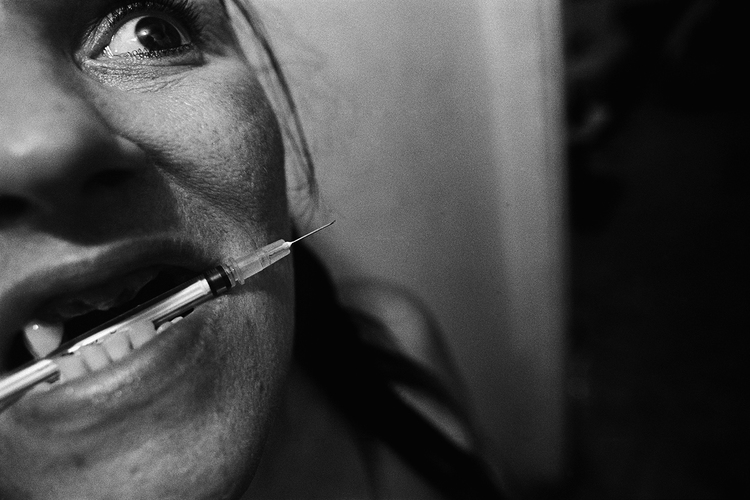
Clark wasn’t the only photographer to represent heroin users this way. Documentary photographer Eugene Richards' 1994 book Cocaine True, Cocaine Blue focused on cocaine use in three inner-city neighborhoods. The book’s cover features an extreme close-up of a woman clenching a syringe between her teeth.
The cover photo for Eugene Richards' Cocaine True, Cocaine Blue dehumanizes the drug user.Eugene Richards, 'Mariella,' East New York, New York, 1992.
The image is arresting and also influenced the way many other photographers have depicted drug users to this day.
Photojournalists working for news agencies such as AP, Getty Images and The Denver Post have recently followed Richards' example and composed images of drug users with syringes in their mouths. In most of these photos, the heroin users' eyes are either partially or completely out of frame or hard to make out in detail.
It’s vital that photographers find more balanced ways of representing drug users, instead of reproducing the same types of stigmatizing images that have existed for decades.
Shocking images certainly provoke reactions. But it’s more important to offer context in order to spark discussions about solutions.
Hearing from the heroin users
In my own effort to produce and share balanced and humanizing images – and to reduce the possibility of misinterpretation and “othering” – I realized the images on their own couldn’t tell the full story. I needed a way to provide context for the viewer.
“The multitude of meanings in a photograph makes it risky, arguably even irresponsible, to trust raw images of marginalization, suffering, and addiction to an often judgmental public,” write Philippe Bourgois and Jeffrey Schonberg in their 2009 book Righteous Dopefiend. “Letting a picture speak its thousand words can results in a thousand deceptions.”
After selecting my final images, I showed them to Marie, Cheryl and Johnny. I wanted to know if they thought the photos accurately represented them, if they thought anything was missing and what they would have done differently if they had taken the photos themselves.
Many of their responses were positive. They thought that in most of the images, I’d accurately represented them. And they had important suggestions. Most of all, they wanted to be seen in the photos as more than just drug users.
I’ve included their most telling comments alongside each of the photos in this story.
Throughout the project, I’d spoken with the subjects about the purpose of the photo essay – to challenge the stereotypes of drug genre photography and to help spread awareness about heroin-assisted treatment.
I often explained to them that their photos would likely be published on the Internet – that police, future employers and others could learn they are heroin users. Despite the risks, the three subjects reiterated that they wanted to take part in the project because they, too, wanted to tell others about heroin-assisted treatment.
I’d been told that after enrolling in the heroin-assisted treatment study, some participants had reconnected with family members, found stable housing and gotten jobs. I hoped that I’d be able to take photos of Marie, Cheryl and Johnny in these types of settings.
However, I quickly learned that this wouldn’t be easy. Two of the three subjects didn’t engage in many other activities beyond self-injecting at the Crosstown clinic three times a day. Outside the clinic, much of their time was spent acquiring and using drugs.
This meant the moments I was able to capture ended up being far less varied than I’d anticipated.
Still, there were revealing moments, like when I managed to photograph Marie traveled across the city by bus to try to find her mother. It was Thanksgiving and she hadn’t seen her mother in over two years. I thought these particular photos might help the viewer understand Marie in a new way: even if people weren’t able to fully understand the depth of Marie’s suffering or the roots of her addiction, everyone knows what it’s like to want to spend the holidays with loved ones.
The greatest challenge I faced was determining how to document two of the subjects' ongoing drug use outside of the heroin-assisted treatment study. I simply couldn’t ignore it because it was a major part of their day-to-day lives. Marie and Cheryl told me that since the study was double-blind, they might not have been receiving the right medication – or high enough doses – to suppress their need to use other drugs. This doesn’t mean heroin-assisted treatment doesn’t work.
When the time came to choose the final photographs, I deliberately left out images that I suspected could be viewed as the most sensational or degrading.
My photo of Cheryl, lit by a candle and injecting drugs into her neck in front of a mirror in her apartment may not appear any less shocking than other drug genre photographers’ images of injection scenes.
However, Cheryl’s own words that accompany the photo provide critical context for the viewer. She explains that she was compelled to buy street drugs and inject into her neck – even though she knew the drugs could be contaminated and possibly kill her – because she was desperate to do whatever she could to feel well, even if this meant risking her life.
In order to see Cheryl as more than a drug user, the viewer needs to know this. Aaron Goodman, Faculty, Journalism and Communication Studies, Kwantlen Polytechnic University
This article was originally published on The Conversation. Read the original article.









































{kind=link}
{kind=link}